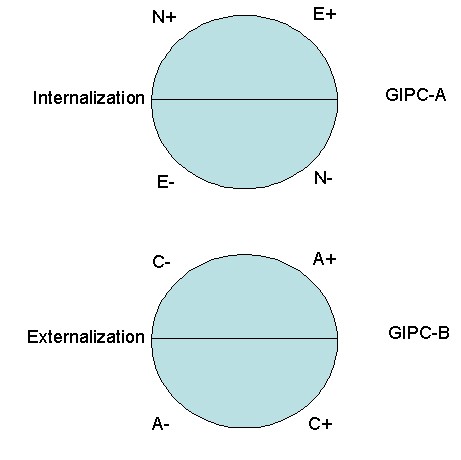
Figure 1. The Generalized Interpersonal Circumplex of Affect (GIPC-A) and Generalized Interpersonal Circumplex of Behavior (GIPC-B)
(2005) Theory & Psychology, 15, 373-399. (PDF)
Classification of Psychopathology: Goals and Methods in an Empirical Approach G. Scott Acton and Jason J. Zodda Rochester Institute of Technology
Author Note
Many have criticized the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994), and few regard it as a vehicle of truth, yet its most serious limitation is that its frank operationism in defining manifest categories has distracted attention from theories about what is going on at the latent level. We sketch a Generalized Interpersonal Theory of Personality and Psychopathology and apply it to interpersonal aspects of depression to illustrate how structural individual differences combine with functional dynamic processes to cause interpersonal behavior and affect. Such a causal account relies on a realist ontology in which manifest diagnoses are only a means to learning about the latent distribution, whether categorical or dimensional. Comorbidity of DSM diagnoses suggests that dimensionality will be the rule, not the exception, with internalization and externalization describing common diagnoses.Keywords: Big Five, circumplex, depression, Dimcat, externalization, internalization
The fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994) virtually holds a monopoly on the classification of psychopathology. Nearly every textbook on abnormal psychology uses DSM classifications so that as a consequence professors will choose the book as a way to prepare their students for successful careers in the helping professions; researchers who study psychopathology know that they probably will not receive grant funding unless they define their terms according to the DSM nomenclature. Because of the extraordinary prominence of the DSM in clinical psychology, psychiatry, and related professions, careful attention to the DSM's philosophical and methodological underpinnings seems warranted.The present article is divided into four parts. The first section provides a clear understanding of how the current DSM has evolved from its predecessors. The second section distinguishes functionalism from structuralism and applies this distinction to the DSM. The third section expands on our alternative to the DSM taxonomy, the Generalized Interpersonal Theory, which incorporates both functionalism and structuralism. The fourth section introduces dimensions as a possibly yet-to-be-realized empirical finding. We distinguish dimensions from categories and show how a dimensional approach is related to fallibilism. In the end, readers will see that a fallibilitic approach to the classification of psychopathology is the only alternative that will engender scientific progress.
In order to understand the context in which we recommend revision of the current psychiatric nosology, it may be useful to take a step back and look at the development of previous classification systems. Before the DSMs were developed, the primary approach to the classification of psychopathology was the “great professor approach” (Kendler, 1990). For centuries, nosologic systems have been developed and promulgated by prominent psychiatrists, including Pinel (1801/1806), Griesinger (1861/1867), Kraepelin (1907/1923), Bleuler (1916/1924), and Schneider (1959). History of Classification in Psychopathology
The DSM-I (APA, 1952) was the American Psychiatric Association's first attempt to develop an official nomenclature for mental disorders. It borrowed heavily from earlier taxonomies developed by the World Health Organization, U.S. Armed Forces, and U.S. Veterans Administration in response to the influx of veterans returning from World War II, many of whom suffered from psychological afflictions, including transient reactions to stress (Widiger, Frances, Pincus, Davis, & First, 1991). For both DSM-I and DSM-II (APA, 1968), empirical validation was limited to an opinion survey of psychiatrists, the “expert consensus approach”--making the diagnostic categories at best "practical kinds" rather than natural kinds (Haslam, 2002)--and the prevailing opinion was that neurotic disorders were rooted in psychodynamic processes, whereas psychotic disorders were rooted in neo-Kraepelinian processes (Kendler, 1990).
One limitation of the early DSMs was the unreliability of their largely impressionistic diagnoses (Helmuth, 2003). Therefore, concurrent with the assumption in psychiatry that biological explanations for disorders would be forthcoming (for a lucid critique of a strong interpretation of this assumption in the "medical model," see Turkheimer, 1998), there was a major attempt in the DSM-III (APA, 1980) to delineate reliable, operationally defined diagnostic categories. Empirical evidence was considered where available, but substantial gaps in knowledge prevented many questions from being informed by empirical evidence, leaving committee members to make recommendations based on their clinical experience (Widiger et al., 1991).
The purpose of the next round of field trials, which informed development of the DSM-III-R (APA, 1987), was to determine the optimal number of indicators to require for maximizing sensitivity and specificity, using clinicians' diagnoses as the criterion (Widiger et al., 1991). No radical alternatives to the existing categorical phenotypes (as they existed in the minds of clinicians) were considered--only minor alterations in the indicators used in their operational definitions. This "tinkering" approach stands in stark contrast to an approach founded on critical realism, in which the growth of knowledge is assumed to require testing competing alternatives. As Lakatos (1970) observed,
The history of science has been and should be a history of competing research programmes (or, if you wish, 'paradigms'), but it has not been and must not become a succession of periods of normal science: the sooner competition starts, the better for progress. (p. 155)To some extent, the process of developing the DSM-IV (APA, 1994) involved the testing of competing alternatives. Specifically, this process involved three steps: (a) approximately 175 literature reviews, (b) reanalyses of existing data sets to generate and evaluate alternative criteria sets, and (c) field trials, including surveys, videotaped reliability studies, and 11 studies to provide reliability and validity data for comparing competing alternative proposals. The field trials involved multiple internal and external validators assessed across multiple sites that provided relevant clinical populations (Widiger et al., 1991). External validators considered to be most important included family history, demographic correlates, biological and psychological tests, environmental risk factors, concurrent symptoms that were not part of the diagnostic criteria being assessed, treatment response, diagnostic stability, and course of illness (Kendler, 1990). Unfortunately, validity requires theoretical understanding of the mechanisms or design properties that cause people to respond as they do rather than amassing external correlates (Embretson, 1983; Borsboom et al., 2004), and theory was not a primary consideration in this process.The DSM-IV revision process resulted in the adoption of (sometimes new) atheoretical, operationally defined categorical phenotypes. A more radical alternative would be to develop theoretically relevant, dimensional endophenotypes (i.e., phenotypes at the latent level). Apparently, the DSM-V is moving in this direction (Helmuth, 2003). Therefore, we propose the development and testing of psychopathological endophenotypes that lie on a continuum with normal personality variation.
Which dimensions of personality are relevant to such an approach? Clark, Watson, and Reynolds (1995) concluded their review of diagnosis and classification of psychopathology by noting that "it is time to halt the general call for dimensional systems and to begin the hard work of developing specific dimensional proposals in targeted domains" (p. 147). Although many personality dimensions have been proposed and should be considered, a large body of research has converged on five personality dimensions, labeled the Big Five--extraversion, agreeableness, conscientiousness, neuroticism, and intellect or openness (e.g., Digman, 1990; Goldberg, 1993; McCrae & Costa, 1997; Wiggins & Pincus, 1992)--which are based on the assumption that those individual differences that are most salient and socially relevant are encoded as terms in the natural language (Saucier & Goldberg, 2001). It seems uncontroversial that most categories of psychopathology are demonstrably salient and socially relevant; thus, they should show systematic relations to the personality variation described in the Big Five. Unfortunately, until now no very elegant method existed for relating manifest categories, such as carefully ascertained DSM-IV diagnoses, to normal personality dimensions, and the typical method has been to develop profile configurations on the Big Five for various diagnoses. Below we discuss a new method for determining whether manifest categories are categorical or dimensional with respect to a given latent dimension. If DSM diagnoses turn out to be dimensional, then the latent dimension could be described as an endophenotype; if they turn out to be dimensional with respect to the Big Five personality dimensions, then each endophenotype can be related to a large body of theorizing within personality psychology, reducing criticisms that the DSM is atheoretical (e.g., Follette, 1996; Follette & Houts, 1996).
Why is it important to identity dimensional endophenotypes instead of continuing to diagnose disorders as operationally defined categories? First, there would be fewer of them. There are approximately 300 diagnostic categories in the DSM-IV (Clark et al., 1995), and researchers have speculated that the DSM-V will contain more (Blashfield & Fuller, 1996). It should certainly be possible to represent this formidable array of categories with a smaller number of basic dimensions that would both accurately reflect the domain and are understandable and useable by clinicians, as they already are to researchers. Second, Eaves (1983) has shown that the difference between scoring a test by counting the number of correct responses (e.g., making a diagnosis by summing symptoms) and more sophisticated methods such as item response theory (e.g., Mellenbergh, 1994; Rijmen, Tuerlinckx, De Boeck, & Kuppens, 2003) are larger than the differences between single gene and polygenic modes of inheritance. Compared to continuous endophenotypes, about 3 times the sample size is needed for equivalent power when a categorical threshold is at the optimal 50 percent; about 10 times the sample size is needed when 10 percent of cases are above the threshold (Neale, Eaves, & Kendler, 1994). Thus, endophenotypes should be an important component of genetic spectrum models of psychopathology. Moreover, a basic finding from quantitative behavior genetics has been that additive genetic variation is not the only influence on behavioral phenotypes--environment may also play an important role, although the specific environments involved are not well-understood (Turkheimer & Waldron, 2000). Many environmental, interpersonal mechanisms of risk and transmission of psychopathology may best be represented by item-explanatory and person-explanatory models at the latent level of endophenotypes (e.g., Acton, Kunz, Wilson, & Hall, 2005; Borsboom et al., 2004; Embretson, 1983; Rijmen et al., 2003; Wilson, 2003). Thus, we see the development of endophenotypes as the wave of the future if descriptive psychopathology is to progress toward explanatory psychopathology.
Several noteworthy critiques of the DSM have been written by functionalists. Functionalism in psychology can be best explained as a within-subject design--the focus is on the distinctiveness of the individual rather than the population (Borsboom, Mellenbergh, & van Herden, 2003). This focus is particularly uncommon in trait psychology (Lamiell, 2000; but see, e.g., Borkenau & Ostendorf, 1998; Fleeson, 2001; Fleeson, Melanos, & Achille, 2002; Watson, Wiese, Vaidya, & Tellegen, 1999). Functionalist writers assert that the DSM is heading in the wrong direction for the future of psychopathology; they note that a vast amount of empirical research concerning behaviorism has corroborated their theory (Follette, 1996; Follette & Houts, 1996). Furthermore, interpersonalists (e.g., Carson, 1991, 1993, 1996) agree with Follette (1996) that research would be more successful if its focus were on behavioral problems. In addition, as discussed below, disorders such as depression seem to necessitate the inclusion of an affective model in addition to a solely behavioral one. Functionalism and Structuralism
A second approach, to which the DSM-IV adheres, is structuralism. In contrast to functionalism, structuralism can be viewed as a between-subjects design; the attention is on differences between groups with and without a diagnosis (or between a group with one diagnosis and a group with another diagnosis) rather than on a particular individual (Borsboom et al., 2003; De Boeck, Wilson, & Acton, 2005). A taxonomy based on structuralism is the backbone of the DSM-IV; this course was chosen by the authors because their focus was on reliability, not validity. Validity can be achieved by providing a theoretical model (Embretson, 1983; Wilson, 2003) that explains either item differences or person differences; the latter can include either differences between persons in traits at one time or differences within persons in states across time. For example, Acton et al. (2005) provided an item-explanatory model to explain the domain of symptoms of internalization. DSM symptoms can be thought of as items in need of explanation--they do not explain anything themselves. Because symptoms define groups of persons (diagnostic groups), we refer to the DSM taxonomy as structuralist.
The DSM is considered by some to be both dimensional and categorical, rather than solely categorical. The argument is that although the DSM is a categorical taxonomy, its symptoms are commonly used to create dimensional measures (e.g., the Beck Depression Inventory). In one sense, symptom counts might be considered dimensional, yet they exist entirely at the manifest level. As the well-known problem of underdetermination (i.e., infinitely many curves can be drawn through the same data points) suggests, manifest dimensions do not necessarily imply latent dimensions; rather, latent dimensions imply certain patterns of symptom endorsement, which may or may not fit the observed data. If a latent dimension fits the data, then the latent dimension can be interpreted as an unobserved entity (Hacking, 1983) that causes the pattern of symptom endorsement.
Latent variables are entities that cause manifest behaviors (Borsboom & Mellenbergh, 2004; Borsboom et al., 2003, 2004). The DSM focuses solely on the manifest level and not the latent level in response to the manual's attachment to reliability and its disregard for explanatory models that could yield validity. Latent variables are not fictitious; the problem is locating them (Michell, 1994, 1997). Identifying a latent variable presupposes a fallibilist epistemology and a realist ontology (Borsboom & Mellenbergh, 2004; Borsboom et al., 2003, 2004). We do not propose that the DSM withdraw from structuralism and become a functionalist taxonomy. Rather, we propose that the ideal is to integrate structuralism and functionalism. There has yet to be a DSM that integrates structuralist and functionalist taxonomy. It is time for a change.
This section discusses the Generalized Interpersonal Theory of Personality and Psychopathology (GIPT). The GIPT is included in this critique of the DSM to illustrate an integration of structuralism and functionalism. Specifically, the GIPT includes both structural and dynamic models, which are used to explain how depression precipitates interpersonal rejection and how expressed emotion precipitates relapse to depression. The Generalized Interpersonal Theory of Personality and Psychopathology
The GIPT provides a framework for understanding the way individuals interact with one another. It is a generalized and distinct form of classical interpersonal theory (e.g., Acton & Revelle, 2002, 2004; Carson, 1969; Horowitz, 2004; Kiesler, 1983; Leary, 1957; Wiggins, Phillips, & Trapnell, 1989), including two additional Big Five personality traits, explaining each trait in terms of affective consequences for the self or others, and predicting affect and behavior in interpersonal interactions based in part on predisposing Big Five personality traits. Because of the growing consensus that the Big Five personality traits are necessary to describe personality across many cultures (e.g., Digman, 1990; Goldberg, 1993; McCrae & Costa, 1997; Saucier & Goldberg, 2001; Wiggins & Pincus, 1992), these traits figure prominently in the GIPT. The Big Five appear to apply not only to between-subjects individual differences but also to within-subject personality processes (e.g., Borkenau & Ostendorf, 1998; Fleeson, 2001; Fleeson et al., 2002; Watson et al., 1999). Only four Big Five personality traits are included in the theory--extraversion, neuroticism, agreeableness, and conscientiousness--because openness or intellect does not appear to have direct affective consequences for the self or others (Yik & Russell, 2001), because it appears to be the least cross-culturally generalizable of the Big Five (Saucier & Goldberg, 2001), and because it appears to have limited relevance to psychopathology (O'Connor & Dyce, 1998; Widiger, 1993).
Internalization and externalization are key constructs in the GIPT. Internalization (feeling bad) describes the comorbidity of unipolar mood and anxiety disorders (e.g., Acton et al., 2005; Hudson et al., 2003; Hudson & Pope, 1990; Kendler, Neale, Kessler, Heath, & Eaves, 1992; Kendler, Prescott, Myers, & Neale, 2003; Krueger, 1999; Krueger & Finger, 2001; Krueger, Caspi, Moffitt, & Silva, 1998; Krueger, Chentsova-Dutton, Markon, Goldberg, & Ormel, 2003; Lahey et al., 2004; Vollebergh et al., 2001), whereas externalization (making others feel bad) describes the comorbidity of antisocial and substance use disorders and impulsivity/disinhibition (e.g., Acton, 2003; Burt, Krueger, McGue, & Iacono, 2001, 2003; Cooper, Wood, Orcutt, & Albino, 2003; Hicks, Krueger, Iacono, McGue, & Patrick, 2004; Iacono, Carlson, Malone, & McGue, 2002; Kendler et al., 2003; Krueger, 1999; Krueger et al., 1998; Krueger et al., 2003; Sher, Bartholow, & Wood, 2000; Sher & Trull, 1994; Lahey et al., 2004; Vollebergh et al., 2001). According to the GIPT, internalization represents a combination of neuroticism and introversion, whereas externalization represents a combination of disagreeableness and non-conscientiousness (cf. Hofstee, De Raad, & Goldberg, 1992). Thus defined, internalization and externalization should be systematically related to personality disorders (e.g., Costa & Widiger, 2002; O’Connor & Dyce, 1998; Widiger, 1993) and to the constructs of many contemporary and historic personality theorists (Appendix).
The GIPT integrates structuralism and functionalism. The structural part of the theory comprises the Generalized Interpersonal Circumplex of Affect (GIPC-A) and the Generalized Interpersonal Circumplex of Behavior (GIPC- B) (Figure 1). Using this model, one can predict a person's affect and behavior in an interpersonal encounter as a function of the person's own predisposing personality traits and the partner's complementary behavior or affect, which arise partially from that person's predisposing personality traits. The functionalist part of the theory comprises the dynamic model or Generalized Interpersonal Principle of Complementarity--a generalization of the classical interpersonal principle of complementarity (e.g., Carson, 1969; Kiesler, 1983; Markey, Funder, & Ozer, 2003)--according to which the probability of experiencing an unpleasantly aroused emotional state that Watson et al. (1999) called negative activation (NA) increases with one's own neuroticism and with a partner's non-conscientiousness, whereas the probability of experiencing a pleasantly aroused emotional state that Watson et al. called positive activation (PA) increases with one's own extraversion and with a partner's agreeableness. Conversely, the probability of exhibiting negative behavior (NB) increases with one's own non-conscientiousness and with a partner's neuroticism, whereas the probability of exhibiting positive behavior (PB) increases with one's own agreeableness and with a partner's extraversion.
The GIPT explains how people's disorders are influenced by the behavioral and emotional expressions of people around them. The explanation involves several testable assumptions. First, based on robust empirical findings (e.g., Krueger, 1999; Vollebergh et al., 2001) and new psychometric methodology (De Boeck et al., 2005), it is contended that common mental disorders can be shown to be extreme manifestations of Big Five personality dimensions. Internalizing disorders (e.g., unipolar mood disorders and anxiety disorders) should turn out to be some combination of neurotic introversion, whereas externalizing disorders (e.g., antisocial personality disorder and substance use disorders) should turn out to be some combination of disagreeable non-conscientiousness. If so, then the dynamic model can be used to predict affect and behavior of persons with these disorders and those in their social environment. Specifically, persons with externalizing disorders are likely to make others feel bad (NA), and persons with internalizing disorders are likely to make other treat them badly (NB). For instance, verbally abusing a neighbor (externalization) makes him or her likely to feel unhappy, and moping around the house (internalization) increases the probability that a spouse will make disparaging comments.
In Figure 1, complementary traits are located at similar positions on each circle. For example, the complement of low conscientiousness is high neuroticism--that is, non-conscientious behavior (e.g., not completing one's duties in a timely manner) causes others to feel distress. In contrast to complementarity, anticomplementarity, or the antidote, can be defined as the opposite of the complement. An anticomplementary response is the treatment for an unwanted trait. For example, high conscientiousness is the antidote for high neuroticism. To help reduce the expression of the unwanted trait of high neuroticism, people in the social environment--friends, family, even strangers--would need to act in a highly conscientious manner, being very careful of their words and actions, walking on eggshells, so to speak.
Depression and Interpersonal Rejection
The relation between depression and interpersonal rejection represents a prime application of the GIPT. In the theory, depression lies at the intersection of high neuroticism and low extraversion. The complement for depression lies at the intersection of low conscientiousness and low agreeableness.According to the tripartite model of anxiety and depression, depression is characterized by low PA and high NA (Clark & Watson, 1991). Persons showing high NA are often overtly distressed, whereas persons showing low PA do not enjoy many activities and rarely feel joy or enthusiasm. These two emotional states, NA and PA, can be seen through the eyes of Big Five theorists as having a basis in neuroticism and extraversion, respectively (Watson, Clark, & Harkness, 1994). Consequently, the conjecture that depression is coterminous with neurotic introversion in the GIPC-A is a plausible, and testable, hypothesis.
Do the people in one's environment play a role in the level of depression one feels? Until the 1970s, psychologists would answer no, assuming that depression is solely an internal factor. These psychologists believed that depression was a schema or personal deficiency. Further, they argued that people in one's environment have nothing to do with one's becoming depressed, nor could they help with its relief (Coyne, 1976b).
Coyne (1976b) adopted an alternative to the common idea that one's depression is based solely on schemas or personal deficiencies; he believed that environment played an important role in causing the disorder. Coyne contended that the depressed person engages others in such a way that their support toward the depressed person is lost.
Coyne (1976b) argued that depressed people often cause the people in their close environment to reject them. In other words, one who originally attempted to help a depressed person winds up acting in a non-conscientious and disagreeable way toward the person. Coyne's theory has been corroborated by many studies (e.g., Coyne, 1976a; Joiner & Coyne, 1999; Nolan, Flynn, & Garber, 2003; Pineles, Mineka, & Nolan, 2004).
In light of Coyne's (1976a, 1976b) arguments, depression is not independent of one's environment. Although one's environment is not the sole cause or cure of the disorder, it does not stand idle while the disorder seizes the person; it plays an active role. Depression is only an extreme manifestation of personality traits that cause the person to provoke others into rejection. According to the dynamic aspect of the GIPT, this phenomenon is expected. High NA and low PA (depression) trigger people in the environment to behave in a non-conscientiousness, disagreeable manner.
Depression and Expressed Emotion
The relation between expressed emotion and depression is a second application of the GIPT; expressed emotion is complementary to depression. As noted before, depression in the GIPT arises from high neuroticism and low extraversion, expressed through high NA and low PA. Consequently, the complement of depression is low conscientiousness and low agreeableness, expressed through high NB and low PB. Therefore, expressed emotion will have to be revealed as a non-conscientious and disagreeable act.Expressed emotion is a measure of the extent to which a family member or friend of a psychiatric patient talks in a critical, hostile, or emotionally over-involved manner about the patient. Expressed emotion is not a characteristic of the patient; rather, it exclusively pertains to the people close to the patient (Hooley & Gotlib, 2000).
Criticalness, the first aspect of expressed emotion, is when friends or family members of patients act disagreeable by using critical remarks, either explicitly or implicitly, which suggest disapproval of the patient's actions (Hooley & Gotlib, 2000). An example of criticalness is a patient's family member or friend exclaiming, "It really irritates me when he just sits around the house all day doing nothing but watching television." As related to the Big Five factors of personality, criticalness is acting disagreeable.
Hostility, the second aspect of expressed emotion, is a much more severe use of criticism. Hostility can best be defined as when family members or friends of the patient criticize the patient for behaving badly because of the patient's internal characteristics (Hooley & Gotlib, 2000). Hostility is thus an extreme manifestation of disagreeableness. An example of hostility would be a friend or family member exclaiming, "Joe, you are liar--I can't trust anything that comes out of your dirty mouth!" Hostility is expressed when one blames a patient's condition on a character flaw.
Emotional over-involvement, the third aspect of expressed emotion, is an excessive and disproportionate involvement in the patient's life. It is more likely to be expressed by family members than by friends. Emotionally over-involved relatives render self-sacrificing responses to the patient's illness, overprotection of the patient, and extreme worry when the patient is not around them (Hooley & Gotlib, 2000). Such behavior can be characterized as an extreme manifestation of sympathy, which Hofstee et al. (1992) showed to be partially a manifestation of non-consciousness. Emotional over-involvement belittles patients, enticing them to feel that without the relatives' presence and support, they will break down. An example of an emotionally over-involved family member is one who says, "I can't leave Joe alone anymore--what if I am not around and he needs me? What then? I can't go to work or to the movies, I have to stay home with Joe all the time."
Expressed emotion is detrimental to the patient's recovery; it has a high correlation with relapse to many psychiatric disorders. Butzlaff and Hooley (1998) found a weighted mean correlation of r = .45 when family members expressed three or more critical comments. This yields a 70% chance of relapse for patients whose families show high levels of expressed emotion (Butzlaff & Hooley, 1998). This evidence strongly corroborates the importance of expressed emotion in relapse to depression.
A diathesis-stress formulation has been proposed for expressed emotion (Hooley & Gotlib, 2000). The diatheses are the underlying personality traits, and the stress is expressed emotion. The idea is that while a patient is recovering from a recent illness, the patient is at high risk for relapsing. If a patient has to deal with expressed emotion on top of the normal after-effects from a recent illness, including medication side effects, then it could be enough to push the patient over the edge into relapse.
With respect to the GIPT, expressed emotion can be understood as a manifestation of low conscientiousness and low agreeableness. Behaving in a critical and hostile manner are disagreeable, and behaving in an emotionally over-involved manner is non-conscientious. Butzlaff and Hooley (1998; Hooley & Teasdale, 1989) have demonstrated that the more expressed emotion a patient's family and friends show, the greater the chance that a patient suffering from depression will relapse. Because expressed emotion represents externalizing behavior, because depression represents internalizing affect, and because expressed emotion causes patients to relapse into depression, expressed emotion can be considered complementary to depression.
In summary, we have proposed a theory, the GIPT, which integrates structuralism and functionalism. We applied the GIPT to two interpersonal aspects of depression: depression precipitating interpersonal rejection and expressed emotion precipitating relapse to depression. In light of its apparent utility in integrating structural and functional aspects of psychopathology, the GIPT can be recommended as one possible theoretical alternative to common DSM diagnoses.
Categories Versus Dimensions: An Empirical Approach
Two Kinds of Categorical Approach
Two kinds of categorical approach should be distinguished: the methodological approach and the empirical approach (Table 1). The methodological approach that underwrites the DSM is operationism (Acton, 1998). Operationism is the methodological dictum that all scientific concepts must be completely defined in terms of the operations or measurements used to recognize them.Operationists with respect to categorization come in two varieties: lumpers and splitters. Lumpers are comfortable with large categories that display considerable within-group heterogeneity. Splitters want to create a new, homogeneous category for every small variation. Both lumpers and splitters prefer a categorical approach based on operationism.
Operationism is a form of infallibilism and is to be contrasted with the alternative epistemological approach, fallibilism. If the arguments in this article are correct, then a dimensional approach based simply on methodological fiat would be no better (and no worse) than the present categorical approach, which itself is based on methodological fiat (De Boeck et al., 2005). For example, a dimensional approach based simply on summing symptom counts would be just as arbitrary and operational as the current categorical approach. The alternative to methodological fiat is fallibilism, which presupposes an interest in the way symptoms and people operate at the latent level of core psychopathological processes (Krueger, 1999) and the possibility that our theoretical models could be wrong (Borsboom et al., 2003).
Fallibilism allows for the discovery of surprising findings, which form the springboard for the growth of knowledge. The nature of discovery, however, is that such findings could crop up--if and only if empirical methods can be employed to test the categorical versus dimensional alternatives. Such methods should be encouraged if a realistic assessment is the goal of our diagnostic scheme, and such methods are irrelevant if realism is not our goal.
Maybe we will turn out to be right in our conjectures every time--but if we are right by fiat, then we should not deceive ourselves that realism is our goal. Rather, we should be content with social constructionism (e.g., Rothbart & Taylor, 1992), because that is the only goal we will have achieved.
Categories Versus Dimensions
Dimensions, factors, and traits are to be contrasted with categories, taxa, and types. Dimensions can be thought of as differences in degree, whereas categories can be thought of as differences in kind (Meehl, 1992). Differences in degree can be large or small--conceptually, infinitely small, as is the case with real numbers on a number line. Differences in kind do not yield to linear conceptualization--for example, blood type is difficult to conceptualize as lying along any continuum. Once the distinction between traits and types is understood, one can still ask whether it is important to draw the distinction conceptually and whether it is possible to detect the distinction empirically.The conceptual importance of the dimensions versus categories question hinges on a particular approach to the classification enterprise. Simply put, the question matters only if one is a realist. Most realists share a belief in the ability of theories to represent the structure of reality accurately--or inaccurately (Devitt, 1991). Critical realists demand that theories not only represent what is known about reality but also what is unknown and yet-to-be-discovered (Lakatos, 1970).
Once one accepts that the dimensions versus categories distinction matters conceptually, there remain two empirical questions: first is the question of whether the distinction matters empirically; second is the question of whether the distinction can be empirically detected. The dimension/category question is vitally important for treatment decisions. Some have suggested that all clinical decisions are ultimately categorical, and therefore, that a categorical model, however arbitrary, is preferable to a dimensional model, however valid. We regard this assumption as gravely mistaken; rather, we regard a dimensional model of diagnosis as leading directly to a graded treatment decision. The most common approach to medical treatment is a stepped-care model, in which the least costly or invasive procedure that is likely to be effective is provided first. Thus, the decision is not whether to treat but how to treat. In certain situations, professional intervention may not be feasible, yet other evidence-based treatments may still be available. For example, Bolton et al. (2003) achieved impressive results in a randomized controlled trial of group interpersonal psychotherapy for depression delivered by indigenous, non-professional residents of rural Uganda who received only brief instruction in the approach: after treatment, the odds of major depression in the control group were over 17 times those in the treatment group. This intervention could not have been undertaken if the decision had been "whether to treat" using antidepressants or professional psychotherapy, which are not widely available in rural Uganda. It exemplifies only one of five types of mental health service delivery that may be available to persons for whom pharmacotherapy or psychotherapy are too costly or invasive to be viable: paraprofessionals, partners, peers, paraphernalia, and print (Christensen, Miller, & Muñoz, 1978). Because of the widespread availability of these alternative forms of prevention and treatment, we see the categorical decision "whether to treat" as being peculiarly focused on priorities other than those of patients', whereas the graded decision "how to treat" is focused on all the viable alternatives available for helping patients.
A second reason the dimension/category issue is vitally important is that it addresses the comparability of different groups. For example, some have suggested that students scoring high on the Beck Depression Inventory are not comparable to patients diagnosed with major depression--that these groups are qualitatively distinct--whereas others have argued for the continuity of depression in clinical and nonclinical samples (e.g., Flett, Vredenberg, & Krames, 1997; Vredenburg, Flett, & Krames, 1993; J. Ruscio & Ruscio, 2000). The usefulness of continuous self-report inventories in clinical practice has obvious practical implications (A. M. Ruscio & Ruscio, 2002), whereas the comparability of groups has important implications for research and interpretation of the published literature (cf., Tennen, Hall, & Affleck, 1995). Given that these aspects of the dimension/category question matter so much empirically, it is fortunate that the methods discussed below can answer them in a rather straightforward manner.
In psychology, some of the best work on the detection of latent categories has been done by Meehl (1995, 2004), who has coined his own term for the numerical aspects of category detection: taxometrics. Whereas the nature of taxometric methods such as those developed by Meehl and others has been detailed elsewhere (e.g., De Boeck et al., 2005; Grayson, 1987; Meehl, 1995, 2004), it is important to call attention here to their potential for answering the empirical questions that our conceptual analysis has shown to be so important for those of a realist philosophical persuasion.
The current DSM is a manual consisting of lists of symptoms and manifest categories. The unfortunate dilemma with taxometrics is that the method does not focus on manifest categories--consequently, a latent taxon discovered by taxometrics may bear little resemblance to any preconceived diagnostic category. Therefore, taxometric methods do not "solve" the specific classification problem in psychopathology posed by the DSM categories.
A recently developed conceptual and methodological approach to this problem is the dimension/category framework, or Dimcat (De Boeck et al., 2005). Dimcat distinguishes latent categories from latent dimensions through the analysis of manifest categories (e.g., diagnoses) and their indicators (e.g., symptoms). Using Dimcat, manifest categories can be explained in terms of latent categories or latent dimensions. Theoretical explanation is what validity requires and what the DSM-IV lacks. Dimcat could be used to show that the DSM's current categorical approach is either accurate or mistaken; the latter finding could entail a new approach to the classification of psychopathology built on a dimensional foundation.
The arguments in this article have been motivated by a particular perspective that is an alternative to the DSM approach. Over against the DSM's operationism lies a fallibilist brand of scientific realism that holds as literally true the way of speaking in which it is said that scientific research or clinical experience has discovered a particular disorder or endophenotype. Such discovery arises from theoretically guided explanations of the interrelations of symptoms, disorders, and people. The DSM's exclusive focus on symptoms and diagnoses at the manifest level is a great methodological shortcoming, distracting attention from the core psychopathological processes in which researchers are interested and preventing thoughtful people from taking the DSM's categorical approach altogether seriously when an empirically based dimensional approach presents such a fruitful alternative.
Table 1. Approaches to the Classification of Psychopathology
Categories Dimensions Methodological Approach Operationism Manifest Categories Sum Scores Lumpers Large Heterogeneous Categories With Highly Sensitive Indicators Splitters Small Homogeneous Categories With Highly Specific Indicators Empirical Approach Taxometrics Latent Taxa No Latent Taxa Dimcat Manifest Categories Categorical at Latent Level Manifest Categories Dimensional at Latent Level Within-Category Homogeneity Present Absent Between-Category Qualitative Differences Present Absent Abrupt Between-Category Differences Present Absent
Figure 1. The Generalized Interpersonal Circumplex of Affect (GIPC-A) and Generalized Interpersonal Circumplex of Behavior (GIPC-B)
Appendix: Theorists Table
Theorists
High Internalization
Low Internalization
High Externalization
Low Externalization
Feeling Bad Feeling Good Making Others Feel Bad Making Others Feel Good Elliot & Thrash (2002) Low Approach Temperament High Approach Temperament Elliot & Thrash (2002) High Avoidance Temperament Low Avoidance Temperament Watson et al. (1999) Low PA High PA Watson et al. (1999) High NA Low NA Hofstee et al. (1992) I- I- (Shyness) I+ I+ (Gregariousness) II- II- (Unsympatheticness) II+ II+ (Understanding) Hofstee et al. (1992) I- IV- (Lack of Poise) I+ IV+ (Poise) II- III- (Immorality) II+ III+ (Morality) Hofstee et al. (1992) IV- I- (Unhappiness) IV+ I+ (Happiness) III- II- (Unreliability) III+ II+ (Dutifulness) Hofstee et al. (1992) IV- IV- (Instability) IV+ IV+ (Stability) III- III- (Unconscientiousness) III+ III+ (Conscientiousness) Eysenck (1992) High Psychoticism Low Psychoticism Eysenck & Eysenck (1985) Low Extraversion High Extraversion Eysenck & Eysenck (1985) High Neuroticism Low Neuroticism Wiggins (1991) Low Agency High Agency Low Communion High Communion Bartholomew & Horowitz (1991) High Dependence / Negative Model of Self Low Dependence / Positive Model of Self High Avoidance / Negative Model of Other Low Avoidance / Positive Model of Other Spielberger et al. (1988) High Anger-In Low Anger-In High Anger-Out Low Anger-Out Caspi et al. (1987, 1988) High Shyness Low Shyness High Explosiveness Low Explosiveness Cloninger (1987) High Harm Avoidance Low Harm Avoidance High Novelty Seeking Low Novelty Seeking McAdams (1985) Low Power Motivation High Power Motivation Low Intimacy Motivation High Intimacy Motivation Beck (1983) High Sociotropy Low Sociotropy Low Sociotropy High Sociotropy Beck (1983) High Autonomy Low Autonomy High Autonomy Low Autonomy Gray (1982) High Anxiety / High Behavioral Inhibition Low Anxiety / Low Behavioral Inhibition Hogan (1982) Low Achieving Status High Achieving Status Low Maintaining Popularity High Maintaining Popularity Blatt et al. (1976) High Dependency Low Dependency Low Dependency High Dependency Blatt et al. (1976) High Self-Criticism Low Self-Criticism High Self-Criticism Low Self-Criticism Bem (1974) Low Masculinity High Masculinity Low Femininity High Femininity Skinner (1971) Low Socialization High Socialization Maslow (1962) Low Self-Actualization High Self-Actualization Rogers (1961) Low Personal Growth High Personal Growth Leary (1957) Low Dominance High Dominance Low Love High Love Sullivan (1953) Low Need for Power High Need for Power Low Need for Tenderness High Need for Tenderness Erickson (1950) Low Autonomy High Autonomy Low Basic Trust High Basic Trust Horney (1945) High Moving Away Low Moving Away High Moving Against Low Moving Against Rank (1945) Low Individualization High Individualization Low Union High Union Fromm (1941) Low Separate Identity High Separate Identity Low Oneness With World High Oneness With World Adler (1939) Low Superiority Striving High Superiority Striving Low Social Interest High Social Interest Freud (1930) Problems With Work Able to Work Problems With Love Able to Love High Internalization
Low Internalization
High Externalization
Low Externalization
Lahey et al. (2004) Depression Conduct Disorder Lahey et al. (2004) Overanxious Disorder Lahey et al. (2004) Social Anxiety Lahey et al. (2004) Separation Anxiety Disorder Hicks et al. (2004) Conduct Disorder Hicks et al. (2004) Antisocial Personality Disorder Hicks et al. (2004) Alcohol Dependence Hicks et al. (2004) Drug Dependence Cooper et al. (2003) Substance Use Cooper et al. (2003) Delinquency Cooper et al. (2003) Problematic Sexual Behavior Cooper et al. (2003) Educational Underachievement Kendler et al. (2003) Major Depression Alcohol Dependence Kendler et al. (2003) Generalized Anxiety Disorder Other Drug Abuse or Dependence Kendler et al. (2003) Panic Disorder Adult Antisocial Behavior Kendler et al. (2003) Animal Phobia Conduct Disorder Kendler et al. (2003) Situational Phobia Krueger et al. (2003) Depression Hazardous Use of Alcohol Krueger et al. (2003) Anxious Worry Krueger et al. (2003) Anxious Arousal Krueger et al. (2003) Neurasthenia Krueger et al. (2003) Somatization Krueger et al. (2003) Hypochondriasis Burt et al. (2001, 2003) Attention-Deficit Hyperactivity Disorder Burt et al. (2001, 2003) Oppositional Defiant Disorder Burt et al. (2001, 2003) Conduct Disorder Hudson et al. (2003),
Hudson & Pope (1990)Major Depressive Disorder Hudson et al. (2003),
Hudson & Pope (1990)Dysthymia Hudson et al. (2003),
Hudson & Pope (1990)Generalized Anxiety Disorder Hudson et al. (2003),
Hudson & Pope (1990)Obsessive-Compulsive Disoder Hudson et al. (2003),
Hudson & Pope (1990)Panic Disorder Hudson et al. (2003),
Hudson & Pope (1990)Social Phobia Hudson et al. (2003),
Hudson & Pope (1990)Bulimia Nervosa Hudson et al. (2003),
Hudson & Pope (1990)Attention-Deficit/Hyperactivity Disoder Hudson et al. (2003),
Hudson & Pope (1990)Posttraumatic Stress Disorder Hudson et al. (2003),
Hudson & Pope (1990)Cataplexy Hudson et al. (2003),
Hudson & Pope (1990)Fibromyalgia Hudson et al. (2003),
Hudson & Pope (1990)Migraine Hudson et al. (2003),
Hudson & Pope (1990)Irritable Bowel Syndrome Hudson et al. (2003),
Hudson & Pope (1990)Premenstrual Dysphoric Disorder Krueger et al. (2002) Alcohol Dependence Krueger et al. (2002) Drug Dependence Krueger et al. (2002) Adolescent Antisocial Behavior Krueger et al. (2002) Conduct Disorder Krueger et al. (2002) Low Constraint High Constraint Vollebergh et al. (2001) Major Depressive Episode Alcohol Dependency Vollebergh et al. (2001) Dysthymia Drug Dependency Vollebergh et al. (2001) Generalized Anxiety Disorder Vollebergh et al. (2001) Social Phobia Vollebergh et al. (2001) Simple Phobia Vollebergh et al. (2001) Agoraphobia Vollebergh et al. (2001) Panic Disorder Krueger (1999) Major Depressive Episode Alcohol Dependence Krueger (1999) Dysthymia Drug Dependence Krueger (1999) Generalized Anxiety Disorder Antisocial Personality Disorder Krueger (1999) Simple Phobia Krueger (1999) Social Phobia Krueger (1999) Agoraphobia Krueger (1999) Panic Disorder Krueger et al. (1998) Major Depressive Episode Alcohol Dependence Krueger et al. (1998) Dysthymia Marijuana Dependence Krueger et al. (1998) Generalized Anxiety Disorder Conduct Disorder Krueger et al. (1998) Agoraphobia Krueger et al. (1998) Social Phobia Krueger et al. (1998) Simple Phobia Krueger et al. (1998) Obsessive-Compulsive Disorder O'Connor & Dyce (1998) Avoidant Personality Disorder Histrionic Personality Disorder Antisocial Personality Disorder Compulsive Personality Disorder O'Connor & Dyce (1998) Dependent Personality Disorder Narcissistic Personality Disorder O'Connor & Dyce (1998) Schizoid Personality Disorder O'Connor & Dyce (1998) Schizotypal Personality Disorder Schizotypal Personality Disorder O'Connor & Dyce (1998) Paranoid Personality Disoder Paranoid Personality Disoder O'Connor & Dyce (1998) Borderline Personality Disorder Borderline Personality Disorder O'Connor & Dyce (1998) Passive-Aggressive Personality Disorder Passive-Aggressive Personality Disorder Butzlaff & Hooley (1998) Mood Disoders Expressed Emotion Butzlaff & Hooley (1998) Eating Disorders Expressed Emotion Coyne (1976a, 1976b) Depression Interpersonal Rejection High Internalization
Low Internalization
High Externalization
Low Externalization
Acton, G. S. (1998). Classification of psychopathology: The nature of language. The Journal of Mind and Behavior, 19, 243-256. References
Acton, G. S. (2003). Measurement of impulsivity in a hierarchical model of personality traits: Implications for substance use. Substance Use & Misuse, 38, 67-83.
Acton, G. S., Kunz, J. D., Wilson, M., & Hall, S. M. (2005). The construct of internalization: Conceptualization, measurement, and prediction of smoking treatment outcome. Psychological Medicine, 35, 395-408.
Acton, G. S., & Revelle, W. (2002). Interpersonal personality measures show circumplex structure based on new psychometric criteria. Journal of Personality Assessment, 79, 456-481.
Acton, G. S., & Revelle, W. (2004). Evaluation of ten psychometric criteria for circumplex structure. Methods of Psychological Research, 9, 1-27.
Adler, A. (1939). Social interest. New York: Putnam.
American Psychiatric Association. (1952). Diagnostic and statistical manual of mental disorders (1st ed.). Washington, DC: Author.
American Psychiatric Association. (1968). Diagnostic and statistical manual of mental disorders (2nd ed.). Washington, DC: Author.
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (Rev. 3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four-category model. Journal of Personality and Social Psychology, 61, 226-244.
Beck, A. T. (1983). Cognitive therapy of depression: New perspectives. In P. J. Clayton & J. E. Barrett (Eds.), Treatment of depression: Old controversies and new approaches (pp. 265-290). New York: Raven.
Bem, S. L. (1974). The measurement of psychological androgyny. Journal of Consulting and Clinical Psychology, 42, 155-162.
Blashfield, R. K., & Fuller, A. K. (1996). Predicting the DSM-V. Journal of Nervous and Mental Disease, 186, 244-246.
Blatt, S. J., D'Afflitti, J. P., & Quinlan, D. M. (1976). Experiences of depression in normal young adults. Journal of Abnormal Psychology, 85, 383-389.
Bleuler, E. (1924). Textbook of psychiatry (A. A. Brill, Trans.). New York: Macmillan. (Original work published 1916)
Bolton, P., Bass, J., Neugebauer, R., Verdeli, H., Clougherty, K. F., Wickramaratne, P., Speelman, L., Ndogoni, L., & Weissman, M. (2003). Group interpersonal psychotherapy for depression in rural Uganda: A randomized controlled trial. JAMA: Journal of the American Medical Association, 289, 3117-3124.
Borkenau, P., & Ostendorf, F. (1998). The Big Five as states: How useful is the five-factor model to describe intraindividual variations over time? Journal of Research in Personality, 32, 202-221.
Borsboom, D., & Mellenbergh, G. J. (2004). Why psychomerics is not pathological: A comment on Michell. Theory & Psychology, 14, 105-120.
Borsboom, D., Mellenbergh, G. J., & van Heerden, J. (2003). The theoretical status of latent variables. Psychological Review, 110, 203-219.
Borsboom, D., Mellenbergh, G. J., & van Heerden, J. (2004). The concept of validity. Psychological Review, 111, 1061-1071.
Burt, S. A., Krueger, R. F., McGue, M., & Iacono, W. G. (2001). Sources of covariation among attention-deficit hyperactivity disorder, oppositional defiant disorder, and conduct disorder: The importance of shared environment. Journal of Abnormal Psychology, 110, 516-525.
Burt, S. A., Krueger, R. F., McGue, M., & Iacono, W. G. (2003). Parent-child conflict and the comorbidity among childhood externalizing disorders. Archives of General Psychiatry, 60, 505-513.
Butzlaff, R. L., & Hooley, J. M. (1998). Expressed emotion and psychiatric relapse: A meta-analysis. Archives of General Psychiatry, 55, 547-552.
Carson, R. C. (1969). Interaction concepts of personality. Chicago: Aldine.
Carson, R. C. (1991). Dilemmas in the pathway of the DSM-IV. Journal of Abnormal Psychology, 100, 302-307.
Carson, R. C. (1993). Can the Big Five help salvage the DSM? Psychological Inquiry, 4, 98-100.
Caspi, A., Elder, G. H., Jr., & Bem, D. J. (1987). Moving against the world: Life-course patterns of explosive children. Developmental Psychology, 23, 308-313.
Caspi, A., Elder, G. H., Jr., & Bem, D. J. (1988). Moving away from the world: Life-course patterns of shy children. Developmental Psychology, 24, 824-831.
Christensen, A., Miller, W. R., & Muñoz, R. F. (1978). Paraprofessionals, partners, peers, paraphernalia, and print: Expanding mental health service delivery. Professional Psychology: Research and Practice, 9, 249-270.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100, 316-336.
Clark, L. A., Watson, D., & Reynolds, S. (1995). Diagnosis and classification of psychopathology: Challenges to the current system and future directions. Annual Review of Psychology, 46, 121-153.
Cloninger, C. R. (1987). A systematic method for description and classification of personality variants: A proposal. Archives of General Psychiatry, 44, 573-588.
Cooper, M. L, Wood, P. K., Orcutt, H. K., & Albino, A. (2003). Personality and the predisposition to engage in risky or problem behaviors during adolescence. Journal of Personality and Social Psychology, 84, 390-410.
Costa, P. T., Jr., & Widiger, T. A. (Eds., 2002). Personality disorders and the five-factor model of personality (2nd ed.). Washington, DC: American Psychological Association.
Coyne, J. C. (1976a). Depression and the response of others. Journal of Abnormal Psychology, 85, 186–193.
Coyne, J. C. (1976b). Toward an interactional description of depression. Psychiatry, 39, 28-40.
De Boeck, P., Wilson, M., & Acton, G. S. (2005). A conceptual and psychometric framework for distinguishing categories and dimensions. Psychological Review, 112, 129-158.
Devitt, M. (1991). Realism and truth (2nd ed.). Princeton, NJ: Princeton University Press.
Digman, J. M. (1990). Personality structure: Emergence of the five-factor model. Annual Review of Psychology, 41, 417-440.
Eaves, L. J. (1983). Errors of inference in the detection of major gene effects on psychological test scores. American Journal of Human Genetics, 35, 1179-1189.
Elliot, A. J., & Thrash, T. M. (2002). Approach-avoidance motivation in personality: Approach and avoidance temperaments and goals. Journal of Personality and Social Psychology, 82, 804-818.
Embretson, S. E. (1983). Construct validity: Construct representation versus nomothetic span. Psychological Bulletin, 93, 179-197.
Erickson, E. (1950). Childhood and society. New York: Norton.
Eysenck, H. J. (1992). The definition and measurement of psychoticism. Personality and Individual Differences, 13, 757-785.
Eysenck, H. J., & Eysenck, M. W. (1985). Personality and individual differences: A natural science approach. New York: Plenum.
Fleeson, W. (2001). Toward a structure- and process-integrated view of personality: Traits as density distributions of states. Journal of Personality and Social Psychology, 80, 1011-1027.
Fleeson, W., Melanos, A. B., & Achille, N. M. (2002). An intraindividual process approach to the relationship between extraversion and positive affect: Is acting extraverted as "good" as being extraverted? Journal of Personality and Social Psychology, 83, 1409-1422.
Flett, G. L., Vredenberg, K., & Krames, L. (1997). The continuity of depression in clinical and nonclinical samples. Psychological Bulletin, 121, 395-416.
Follette, W. C. (1996). Introduction to the special section on the development of theoretically coherent alternatives to the DSM system. Journal of Consulting and Clinical Psychology, 64, 1117-1119.
Follette, W. C., & Houts, A. C. (1996). Models of scientific progress and the role of theory in taxonomy development: A case study of the DSM. Journal of Consulting and Clinical Psychology, 64, 1120-1132.
Freud, S. (1930). Civilization and its discontents. New York: Norton.
Fromm, E. (1941). Escape from freedom. New York: Avon Books.
Goldberg, L. R. (1993). The structure of phenotypic personality traits. American Psychologist, 48, 26-34.
Gray, J. A. (1982). Précis of The neuropsychology of anxiety: An enquiry into the functions of the septo-hippocampal system. Behavioral and Brain Sciences, 5, 469-534.
Grayson, D. A. (1987). Can categorical and dimensional views of psychiatric illness be distinguished? British Journal of Psychiatry, 151, 355-361.
Griesinger, W. (1867). Mental pathology and therapeutics (2nd ed., C. L. Robertson & J. Rutherford, Trans.). London: New Syndenham Society. (Original work published 1861)
Hacking, I. (1983). Representing and intervening: Introductory topics in the philosophy of natural science. New York: Cambridge University Press.
Haslam, N. (2002). Kinds of kinds: A conceptual taxonomy of psychiatric categories. Philosophy, Psychiatry & Psychology, 9, 203-217.
Helmuth, L. (2003). In sickness or in health? Science, 302, 808-810.
Hicks, B. M., Krueger, R. F., Iacono, W. G., McGue, M., & Patrick, C. J. (2004). Family transmission and heritability of externalizing disorders: A twin-family study. Archives of General Psychiatry, 61, 922-928.
Hofstee, W. K. B., De Raad, B., & Goldberg, L. R. (1992). Integration of the Big Five and circumplex approaches to trait structure. Journal of Personality and Social Psychology, 63, 146-163.
Hogan, R. (1982). A socioanalytic theory of personality. Nebraska Symposium on Motivation, 30, 55-89.
Hooley, J. M., & Gotlib, I. H. (2000). A diathesis-stress conceptualization of expressed emotion and clinical outcome. Applied & Preventive Psychology, 9, 135-151.
Hooley, J. M., & Teasdale, J. D. (1989). Predictors of relapse in unipolar depressives: Expressed emotion, marital distress, and perceived criticism. Journal of Abnormal Psychology, 98, 229-235.
Horney, K. (1945). Our inner conflicts. New York: Norton.
Horowitz, L. M. (2004). Interpersonal foundations of psychopathology. Washington, DC: American Psychological Association.
Hudson, J. I., Mangweth, B., Pope, H. G., Jr., De Col, C., Hausmann, A., Gutweniger, S., Laird, N. M., Biebl, W., & Tsuang, M. T. (2003). Family study of affective spectrum disorder. Archives of General Psychiatry, 60, 170-177.
Hudson, J. I., & Pope, H. G., Jr. (1990). Affective spectrum disorder: Does antidepressant response identify a family of disorders with a common pathophysiology? American Journal of Psychiatry, 147, 552-564.
Iacono, W. G., Carlson, S. R., Malone, S. M., & McGue, M. (2002). P3 event-related potential amplitude and the risk for disinhibitory disorders in adolescent boys. Archives of General Psychiatry, 59, 750-757.
Joiner, T., & Coyne, J. C. (Eds., 1999). The interactional nature of depression: Advances in interpersonal approaches. Washington, DC: American Psychological Association.
Kendler, K. S. (1990). Toward a scientific psychiatric nosology: Strengths and limitations. Archives of General Psychiatry, 47, 969-973.
Kendler, K. S., Neale, M. C., Kessler, R. C., Heath, A. C., & Eaves, L. J. (1992). Major depression and generalized anxiety disorder: Same genes, (partly) different environments? Archives of General Psychiatry, 49, 716-722.
Kendler, K. S., Prescott, C. A., Myers, J., & Neale, M. C. (2003). The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Archives of General Psychiatry, 60, 929-937.
Kiesler, D. J. (1983). The 1982 interpersonal circle: A taxonomy for complementarity in human transactions. Psychological Review, 90, 185-214.
Kraepelin, E. (1923). Clinical psychiatry: A textbook for students and physicians (7th ed., A. F. Diefendorf, Trans.). New York: Macmillan. (Original work published 1907)
Krueger, R. F. (1999). The structure of common mental disorders. Archives of General Psychiatry, 56, 921-926.
Krueger, R. F., Caspi, A., Moffitt, T. E., & Silva, P. E. (1998). The structure and stability of common mental disorders (DSM-III-R): A longitudinal-epidemiological study. Journal of Abnormal Psychology, 107, 216-227.
Krueger, R. F., Chentsova-Dutton, Y. E., Markon, K. E., Goldberg, D., & Ormel, J. (2003). A cross-cultural study of the structure of comorbidity among common psychopathological syndromes in the general health care setting. Journal of Abnormal Psychology, 112, 437-447.
Krueger, R. F., & Finger, M. S. (2001). Using item response theory to understand comorbidity among anxiety and unipolar mood disorders. Psychological Assessment, 13, 140-151.
Krueger, R. F., Hicks, B. M., Patrick, C. J., Carlson, S. R., Iacono, W. G., & McGue, M. (2002). Etiologic connections among substance dependence, antisocial behavior, and personality: Modeling the externalizing spectrum. Journal of Abnormal Psychology, 111, 411-424.
Lahey, B. B., Applegate, B., Waldman, I. D., Loft, J. D., Hankin, B. L., & Rick, J. (2004). The structure of child and adolescent psychopathology: Generating new hypotheses. Journal of Abnormal Psychology, 113, 358-385.
Lakatos, I. (1970). Falsification and the methodology of scientific research programmes. In I. Lakatos & A. Musgrave (Eds.), Criticism and the growth of knowledge (pp. 91-196). New York: Cambridge University Press.
Lamiell, J. T. (2000). A periodic table of personality elements? The "Big Five" and trait "psychology" in critical perspective. Journal of Theoretical & Philosophical Psychology, 20, 1-24.
Leary, T. (1957). Interpersonal diagnosis of personality. New York: Ronald.
Markey, P. M., Funder, D. C., & Ozer, D. J. (2003). Complementarity of interpersonal behaviors in dyadic interactions. Personality and Social Psychology Bulletin, 29, 1082-1090.
Maslow, A. H. (1962). Toward a psychology of being. Oxford, England: Van Nostrand.
McAdams, D. P. (1985). Power, intimacy, and the life story: Psychological inquiries into identity. Homewood, IL: Dow-Jones-Irwin.
McCrae, R. R., & Costa, P. T., Jr. (1997). Personality trait structure as a human universal. American Psychologist, 52, 509-516.
Meehl, P. E. (1992). Factors and taxa, traits and types, differences of degree and differences in kind. Journal of Personality, 60, 117-174.
Meehl, P. E. (1995). Bootstraps taxometrics: Solving the classification problem in psychopathology. American Psychologist, 50, 266-275.
Meehl, P. E. (2004). What's in a taxon? Journal of Abnormal Psychology, 113, 39-43.
Mellenbergh, G. J. (1994). Generalized linear item response theory. Psychological Bulletin, 115, 300-307.
Michell, J. (1994). Numbers as quantitative relations and the traditional theory of measurement. British Journal for the Philosophy of Science, 45, 389-406.
Michell, J. (1997). Quantitative science and the definition of measurement in psychology. British Journal of Psychology, 88, 355-383.
Neale, M. C., Eaves, L. J., & Kendler, K. S. (1994). The power of the classical twin study to resolve variation in threshold traits. Behavior Genetics, 24, 239-258.
Nolan, S. A., Flynn, C., & Garber, J. (2003). Prospective relations between rejection and depression in young adolescents. Journal of Personality and Social Psychology, 85, 745-755.
O'Connor, B. P., & Dyce, J. A. (1998). A test of models of personality disorder configuration. Journal of Abnormal Psychology, 107, 3-16.
Pinel, P. (1806). A treatise on insanity (D. D. Davis, Trans.). Sheffield, England: W. Todd. (Original work published 1801)
Pineles, S. L., Mineka, S., & Nolan, S. A. (2004). Interpersonal appraisals of emotionally distressed persons by anxious and dysphoric individuals. Journal of Anxiety Disorders, 18, 779-797.
Rank, O. (1945). Will therapy and truth and reality. New York: Knopf.
Rijmen, F., Tuerlinckx, F., De Boeck, P., & Kuppens, P. (2003). A nonlinear mixed model framework for item response theory. Psychological Methods, 8, 185-205.
Rogers, C. R. (1961). On becoming a person. Boston: Houghton Miflin.
Rothbart, M., & Taylor, M. (1992). Category labels and social reality: Do we view social categories as natural kinds? In G. R. Semin & K. Fiedler (Eds.), Language, interaction and social cognition (pp. 11-36). London: Sage.
Ruscio, A. M., & Ruscio, J. (2002). The latent structure of analogue depression: Should the Beck Depression Inventory be used to classify groups? Psychological Assessment, 13, 135-145.
Ruscio, J., & Ruscio, A. M. (2000). Informing the continuity controversy: A taxometric analysis of depression. Journal of Abnormal Psychology, 109, 473-487.
Saucier, G., & Goldberg, L. R. (2001). Lexical studies of indigenous personality factors: Premises, products, and prospects. Journal of Personality, 69, 847-880.
Schneider, K. (1959). Clinical psychopathology. New York: Grune & Stratton.
Sher, K. J., Bartholow, B. D., & Wood, M. D. (2000). Personality and substance use disorders: A prospective study. Journal of Consulting and Clinical Psychology, 68, 818-829.
Sher, K. J., & Trull, T. J. (1994). Personality and disinhibitory psychopathology: Alcoholism and antisocial personality disorder. Journal of Abnormal Psychology, 103, 92-102.
Skinner, B. F. (1971). Beyond freedom and dignity. New York: Knopf.
Spielberger, C. D., Krasner, S. S., & Solomon, E. P. (1988). The experience, expression, and control of anger. In M. P. Janisse (Ed.), Health psychology: Individual differences and stress (pp. 89-108). New York: Springer.
Sullivan, H. S. (1953). The interpersonal theory of psychiatry. New York: Norton.
Tennen, H., Hall, J. A., & Affleck, G. (1995). Depression research methodologies in the Journal of Personality and Social Psychology: A review and critique. Journal of Personality and Social Psychology, 68, 870-884.
Turkheimer, E. (1998). Heritability and biological explanation. Psychological Review, 105, 782-791.
Turkheimer, E., & Waldron, M. (2000). Nonshared environment: A theoretical, methodological, and quantitative review. Psychological Bulletin, 126, 78-108.
Vollebergh, W. A. M., Iedema, J., Bijl, R. V., de Graaf, R., Smit, F., & Ormel, J. (2001). The structure and stability of common mental disorders: The NEMESIS study. Archives of General Psychiatry, 58, 597-603.
Vredenburg, K., Flett, G. L., & Krames, L. (1993). Analogue versus clinical depression: A critical reappraisal. Psychological Bulletin, 113, 327-344.
Watson, D., Clark, L. A., & Harkness, A. R. (1994). Structures of personality and their relevance to psychopathology. Journal of Abnormal Psychology, 103, 18-31.
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999). The two general activation systems of affect: Structural findings, evolutionary considerations, and psychobiological evidence. Journal of Personality and Social Psychology, 76, 820-838.
Widiger, T. A. (1993). The DSM-III-R categorical personality disorder diagnoses: A critique and an alternative. Psychological Inquiry, 4, 75-90.
Widiger, T. A., Frances, A. J., Pincus, H. A., Davis, W. W., & First, M. B. (1991). Toward an empirical classification for the DSM-IV. Journal of Abnormal Psychology, 100, 280-288.
Wiggins, J. S. (1991). Agency and communion as conceptual coordinates for the understanding and measurement of interpersonal behavior. In W. M. Grove & D. Cicchetti (Eds.), Thinking clearly about psychology: Essays in honor of Paul Everett Meehl. Vol. 2: Personality and psychopathology (pp. 89-113). Minneapolis, MN: University of Minnesota Press.
Wiggins, J. S., Phillips, N., & Trapnell, P. (1989). Circular reasoning about interpersonal behavior: Evidence concerning some untested assumptions underlying diagnostic classification. Journal of Personality and Social Psychology, 56, 296-305.
Wiggins, J. S., & Pincus, A. L. (1992). Personality: Structure and assessment. Annual Review of Psychology, 43, 473-504.
Wilson, M. (2003). On choosing a model for measuring. Methods of Psychological Research, 8, 1-22.
Yik, M. S. M., & Russell, J. A. (2001). Predicting the Big Two of affect from the Big Five of personality. Journal of Research in Personality, 35, 247-277.
Last modified March 2005
Visited times since July 2001
Comments?
Home to Great Ideas in Personality